
Shoulder Impingement: Internal / Posterior Impingement
Internal Impingement, often refereed to as posterior impingement, typically presents with pain/pinching in the posterior shoulder with the combination of External rotation and Horizontal Abduction regardless of whether the movement is active or passive. It is likely the athlete will feel the posterior shoulder pain at the lay back portion of the throw.

WHY DOES IT OCCUR?
1) The increase in Horizontal Abduction (elbow moving behind shoulders) creates a pinching/closing angle fulcrum of the deep structures of the posterior shoulder (Infraspinatus, Teres Minor, Posterior Labrum).
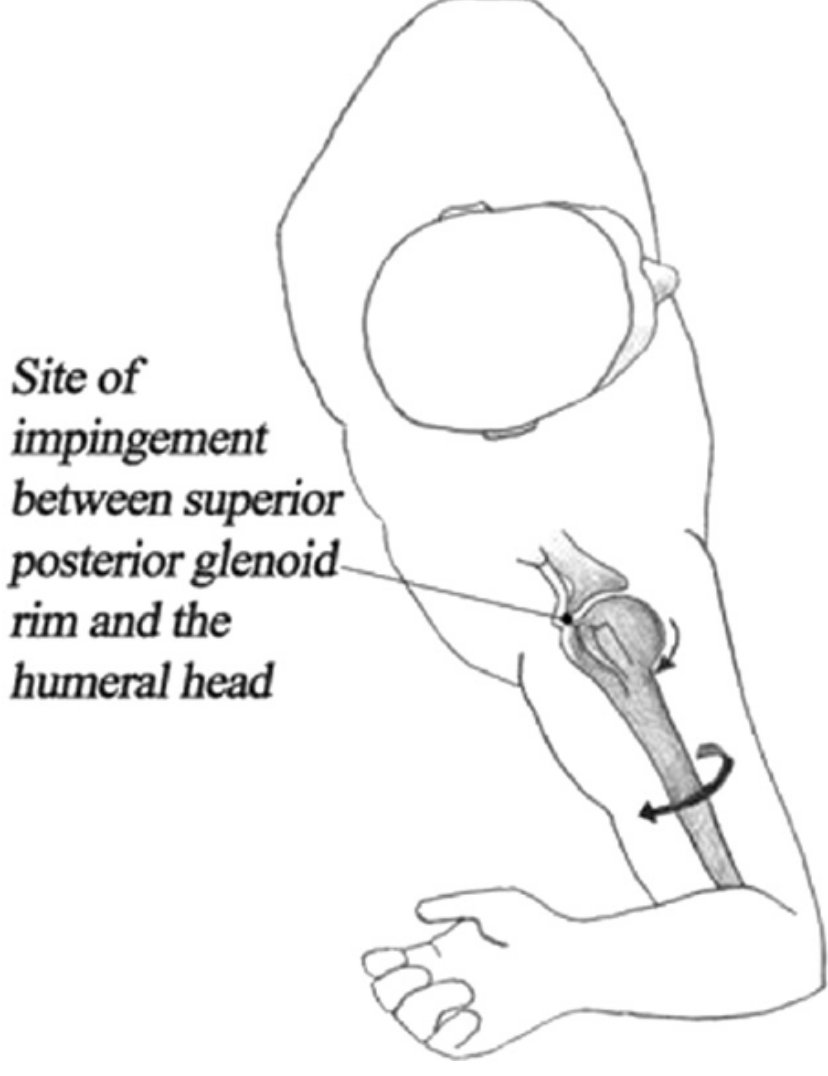
2) Now, add in the Max External Rotation which leads to the bulky greater tuberosity rolling to the back of the shoulder joint, leading to a pinch of the Infraspinatus/Teres Minor tendons into the glenoid rim and labrum
3) When this is done repetitively, those tendons or the labrum will create an inflammatory response and possible damage to the tissue depending on the severity and chronicity
4) Because it is the position and not the contractile force that causes these symptoms, the layback position is often symptomatic regardless on if there is resistance to the movement or not. Muscle testing can commonly test strong with no pain with this condition
ADDRESS THE PROBLEM AT IT’S ROOT
1) Horizontal Abduction is not bad in itself. However, if you cannot make your glenoid (golf tee of the scapula) point behind your shoulders with this motion, you are creating a large pinching fulcrum. Focus on the ability to retract your scapula to midline and on your T Spine/rib mobility in the segments above T7. This will help to orient the Glenoid pointing posterior of midline and keep arm centered in the shoulder joint. We have also talked with Pitching Coaches about the timing of ER and Horizontal Abduction “Loading” and the speed going into layback in the delivery also playing a role in this. This makes a TON of sense, but we will stay in our scope of expertise, which is not pitching mechanics.
2) Increase Scapular Posterior Scapular tilt and T spine extension to spread out where the layback is coming from and disperse the demands of this position to more stable segments
3) Hammering shoulder strength and stability work during this time will also be a crucial factor and one of the foundational component of the rehab process

QUICK TESTS:
1) Have the Athlete bounce into ER with no load or ball and see if a posterior pinching or discomfort is reproduced
2) Bring Elbow in front of shoulder line (Horizontal Adduction), then externally rotate and see if symptoms decrease in comparison
3) FOR CLINICIANS: Perform a posterior humeral Glide with this full layback (similar to Jobe Relocation Test) and see if symptoms decrease
Although these are not “official” diagnostic tests, they are great ways to test your hypothesis if you are thinking the athlete has Internal Impingement.
**This post is for informative purposes only. We recommend seeing a highly knowledgable Medical Professional in your local area if you are dealing with shoulder discomfort